Benign paroxysmal positional vertigo, often abbreviated as BPPV, is a common inner ear disorder that causes brief episodes of dizziness or spinning sensations when your head moves in certain positions. Some of the individuals have unexpected attacks of vertigo, which may interfere with all normal activities in life, such as getting out of bed, looking up, or turning over, and, thus, make life unpredictable and sometimes scary. Understanding benign paroxysmal positional vertigo is essential because it affects millions worldwide and is one of the most treatable forms of vertigo.
If you or a loved one has had dizzy spells or has felt unsteady without an apparent cause, then understanding BPPV can give you the ability to seek out the best available treatments, minimize the pain and discomfort, and live a better quality of life.
Key Takeaways:
- BPPV imparts short, acute dizziness from small crystals in the inner ear.
- Most of the cases can be taken care of by simple repositioning maneuvers.
- Early-diagnosed and treated wounds enhance effective recovery and the avoidance of future attacks.
In the following sections, we will explore what benign paroxysmal positional vertigo is, how doctors diagnose it, and what you can do to get back on your feet quickly.
What Is Benign Paroxysmal Positional Vertigo and How Does It Occur?
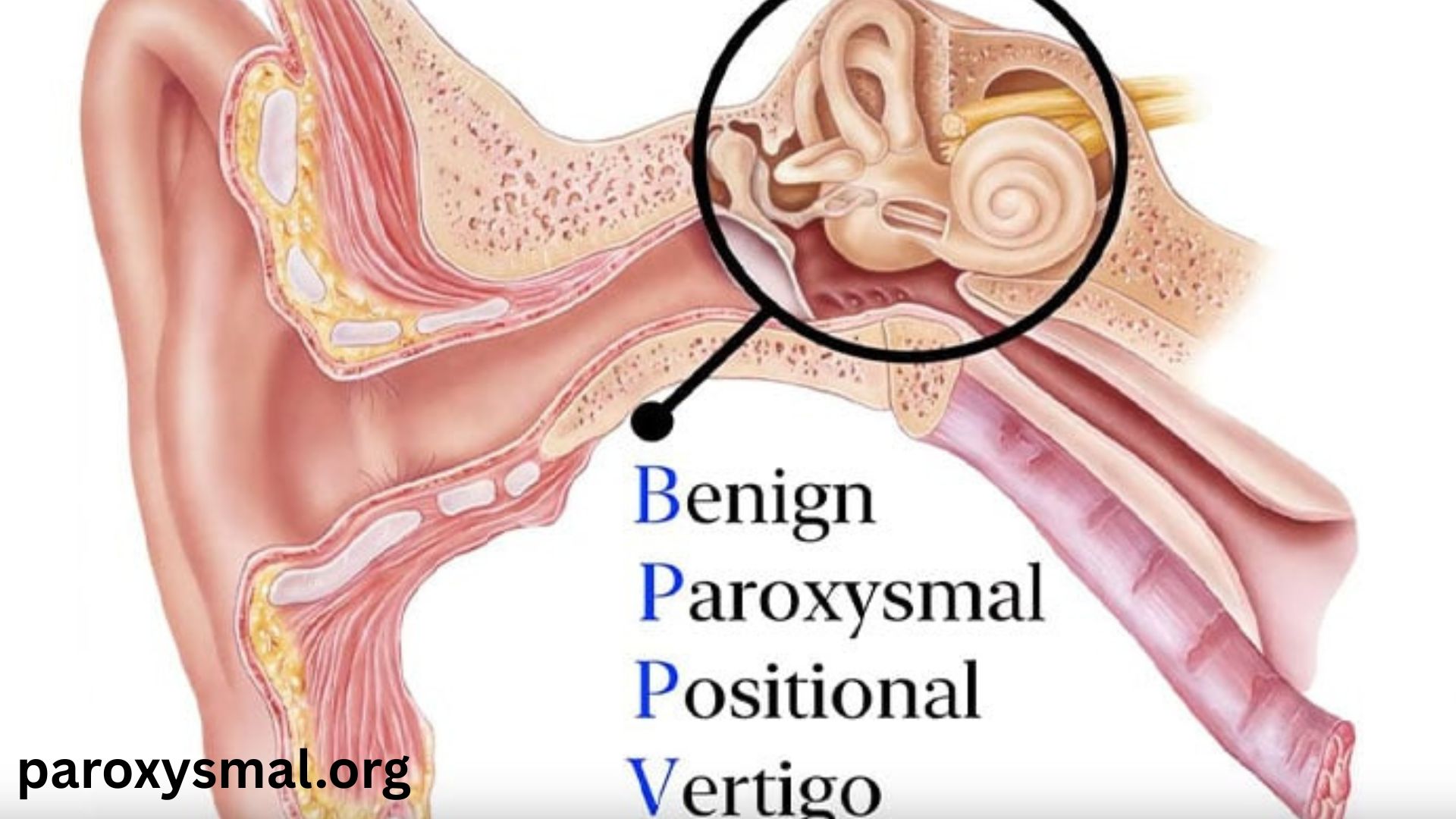
Benign paroxysmal positional vertigo is a disorder related to your vestibular system, the part of your inner ear responsible for balance and spatial orientation. The term benign means it is non-fatal, paroxysmal implies that it occurs suddenly, and finally positional means that the dizzying occurs with certain head positions.
What Causes BPPV?
Depending on the size of the calcium carbonate crystals, they are typically known as otoconia; they tend to stick to a gel-like substance that is found in your ear. In BPPV, the existence of these crystals is dislodged and moves into one or more of the semicircular canals, where it does not belong. These loose crystals slip (and send mixed signals to your brain) when your head moves, messing up the balancing sensors in your inner ear. This causes the feeling of spinning or vertigo.
Risk factors and common causes
Age: BPPV occurs at a higher rate in elderly people as the inner ear structures are degenerated by the natural process.
Trauma may dislodge crystals . Head injuries.
Ear infections and operations: Their ears may be upset with ear infections and operations.
Other vestibular disorders: Conditions like MAtcid ptrM énI brains disease can pose an enhancement.
Example Case
A 67 year old retired teacher, Mrs. Johnson, felt perturbed because she became dizzy at the moment she rolled over in bed. Having experienced a fall once, she came to see an ENT specialist who diagnosed her with BPPV. Her symptoms were cured in a matter of a few days with the help of a simple repositioning treatment, which gave her ample confidence and prevented her falls.
Notes: Diagnosis by a trained healthcare professional is very important to avoid unwanted testing and complications as early as possible.
How Is Benign Paroxysmal Positional Vertigo Diagnosed? Testing the Tests and Symptoms
Your medical history and physical examination, including paying attention to certain head movements resulting in vertigo, are critical in diagnosing BPPV. Specific maneuvers and tools are applied by the doctors to determine the affected semicircular canal.
Popular diagnostic techniques
Dix-Hallpike test: It is the most common test, in which it is rotated so fast and lowered to make the patient experience vertigo, and monitored via eye movement ( nystagmus).
Roll Test: It helps to test horizontal canal BPPV by rolling the head left or right when a person is lying or sitting.
Other examinations: Audiometry can be performed to eliminate the presence of hearing loss or any other ear problem.
The Diagnosis of BPPV Vs Other Causes of Dizziness
Vertigo may be caused by several predisposing conditions, like vestibular neuritis, migraines, or stroke. But the patterns of BPPV instead involve only onlyshort-lastingt (less than 60 seconds) position-induced vertigo and no hearing loss. The difference assists physicians in establishing an appropriate course of action.
Diagnostic Test Undiagnosed Useful Purpose Purpose TBPPV Expected TBPPV Result Result Result Result ALT Text: Table of diagnostic tests, their purpose, and expected result in BPPV.
Dix-Hallpike Test Find the cause-posterior canal BPP. Induce momentary vertigo and nystagmus. This table is the typical BPPV test, the goal of the test, and the predicted result of it
Roll Test Diagnose horizontal canal BPP, V Side-to-side v, vertigo and head-rotating eye movement.nts
Audiometry Test of the hearing is Normal in BPPV
Expert Insight
Dr. Marie Clarke, who is a vestibular specialist, notes, the gold standard to diagnose BPPV accurately is a careful physical examination, including SU, PPA, regardless of underlying disorder. This prevents extra imaging and leads to suitable treatment.
Effective Treatments and Therapies for Benign Paroxysmal Positional Vertigo
The good news is that benign paroxysmal positional vertigo can often be cured or at least significantly improved with simple treatment methods.
Canalith Meeting Maneuvers
These are the main modalities of treatment that try to drive the moved crystals to their native place.
Epley Maneuver: This is the most common and is used most often in the treatment of posterior canal BPPV.
Semont Maneuver: A faster methodology of the head movement performed in the lying position.
Gufoni Maneuver: This is applied to horizontal canal BPPV.
The maneuvers are done by a trained therapist or health care provider, but some patients become skilled enough to do them confidently at home.
Other Treatments and Medication
Drugs such as vestibular suppressants (e.g, meclizine) bring a temporary relief but have no curative effects on BPPV. Minor surgery is uncommonly necessary and d only used on stubborn, severe cases.
- Sudden movement of the head or changes of position.
- Be very careful when leaving the bed or hunching.
- Hydrate and take care of the underlying health issues.
In case of John, age 42, a software engineer who complained of episodes of vertigo in the workplace, as they pulled up to the office. Two sessions of physical therapy involving cthe analith repositioning maneuver resulted in the disappearance of his symptoms, and he was able to tontinue his daily activities without any doubts.
Learning About the Risks and Intervals of Recurrence and How to Get Medical Care
Although BPPV is harmless and is treatable, it may recur or be an indication of more complications. Research indicates that recurrent BPPV occurs at a rate of around fifteen to twenty percent in patients within one year of being treated. Most people are still responsive to repeated maneuvers of repositioning.
The study of BPPV still optimises diagnostic measures, successfully manages interventions, and perceptions of the recurrence.
Emerging Trends
Vestibular integrated vests to monitor balance and early onset symptoms.
Telemedicine of distant diagnosis and controlled movements.
Better imaging modalities ito tovisualize structures of the inner ear.
Data Insights
The American Academy of Otolaryngology argues that the prevalence of BPPV in the general population is up to 2.4 percent per year, which explains the necessity of easy access resources and education campaigns on the topic. When you or a loved one is suddenly dizzy when the head is moved, do not be afraid to turn to one of the healthcare specialists ito findout what can be done. The intervention today helps not only eliminate symptoms but also prevent the recurring fall and non-treated vertigo complications. Be aware, be secure, and get yourself back on track.
The readers who want to know more about the related vestibular disorders should read our elaborate article on labyrinthitis and vestibular rehabilitation therapy for balance disorders.
Conclusion
Benign paroxysmal positional vertigo is a common but highly treatable condition that affects the inner ear’s balance system, producing brief yet disruptive dizzy spells. Knowledge of causes, identification of symptoms, and early diagnosis are important measures to deal with this condition efficiently. Most patients obtain considerable or full relief with easy positioning movement, and resume normal activity rapidly and safely. Keep in mind that though the symptoms might be alarming, BPPV is neither harmful nor life-threatening, and your quality will change for the better at the moment of receiving treatment by a specialist dramatically.
FAQs
Q1: What causes benign paroxysmal positional vertigo?
A: It is precipitated by the dislodgement of small calcium crystals into the inner ear canals, interfering with the signal of the balance.
Q2: What is the length of the BPPV symptoms?
A: The symptoms are short-lived, taking less than a minute, and the symptoms occur after assuming some positions of head positions.
Q3: Can benign paroxysmal positional vertigo go away on its own?
A: In some cases, it can resolve itsel;, however, in most cases, repositioning maneuvers help to improve motor recovery and decrease rates of recurrence.
Q4: Does BPPV alternate with dizziness caused by dehydration/anxiety?
A: No, BPPV is the spinning vertigo, which is provoked by movements of the head, as opposed to general dizziness due to other reasons.
Q5: At what times do I get a doctor in case of vertigo?
A: In case of severe vertigo, persistent vertigo, presence of hearing loss, weakness, or safety issues, head to the doctor.